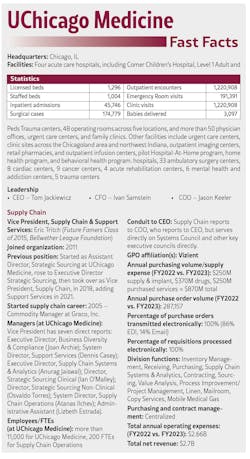
UChicago Medicine supply chain team always on the go

When a healthcare organization nurtures myriad plans and processes fortified by teams of people, outfitted with relevant technology, rooted in customer service, and defined performance measurement parameters, then that organization can navigate around and negotiate through even the most challenging clinical, financial, and operational storms.
Like a global pandemic, for example, which rattled the healthcare industry from 2020 through earlier this year, disrupting supply chains made evident among the burgeoning reports of backorders and stockouts, dealing a crippling (but not fatal) blow to just-in-time distribution.
Some facilities were able to bob and weave, dodge and weather the aftershocks of the pandemic using creative foresight, prudent demand planning, and relationships with alternative and auxiliary suppliers that may have seemed a bit unorthodox.
All about accountability
UCM’s Supply Chain team recognizes accountability as one of the elementary underpinnings of improving performance and maintaining trust with customers.
All sub-teams within the group consistently monitor a number of key metrics and performance indicators across departments, including open orders, orders per day, packages received against purchase orders, fill rates, stockouts, inventory dollars on hand, internal backorders, invoice discrepancies, and days sales outstanding (DSO) for cash flow.
“I do believe these are fundamental KPIs that all supply chains should measure,” said Eric Tritch, UCM’s vice president, Supply Chain & Support Services. “There could be some slight tweaks, but you need measures of your performance to your stakeholders. You need to be laser-focused on how you can make the lives of your patients and end users better and easier. The metrics shared [for HPN’s annual award] were really around clinical supply stocking and inventory management, and the aggressive pursuit of 100% fill rates. However, we have similar metrics around contract cycle time, item add/supplier add cycle time, and value analysis requests. We need to be able to effectively execute our processes and get answers back to requestors to move initiatives forward to lower cost and improve outcomes.”
One of UCM Supply Chain’s notable accomplishments showed declining overall stockout rates (slashed by 50%) while expanding service locations in the two years leading up to the pandemic. How did they do it? By identifying root causes and implementing basic but detailed countermeasures, according to Atanas Ilchev, system director, Supply Chain Operations & Logistics.
“Most of our KPI information is obtained from our inventory management system, including stockout rate, stocking locations, and SKUs in each location,” Ilchev said. “KPIs are fundamental for understanding your performance and charting a course to achieve a target. Countermeasures are established daily [during] our huddle, and through root-causing we perform when we encounter issues. Thorough, fast, and effective root-causing is key to continuous improvement, and we are working with all Supply Chain members daily to be better at this.”

Attainable innovation
A healthcare organization striving to improve efficiency and performance may at first mobilize people before ultimately throwing as much technology into the mix as possible, particularly as budgets permit.
Not UCM.
Being part of a sizeable urban academic institution that may afford the ability to adopt and implement as many high-tech tools as possible, Tritch’s team approached this option with discretion and due diligence.
Rather than fully embrace the latest tech for everything, UCM applies three different tech types to three specific service line areas spanning more than 65,100 item locations supported by 59 full-time equivalents (FTEs) – Med/Surg, which encompass traditional inpatient supply room locations; OR, which involve operating room support for med/surg-type items, such as case picking for preference cards; and Procedural, which support in-patient and outpatient procedures calling for high-dollar, specialized and case-specific materials. Each area uses some combination of tech type, ranging from barcoding on the low-tech side, radiofrequency identification (RFID)-enabled Kanban on the mid-tech side, and individual RFID tagging on the high-tech side, augmented by Tableau dashboards to enable comprehensive and compartmentalized visual analysis.
UCM tracks and measures the bulk of med/surg inventory via Kanban with RFID tags for the majority and barcoding for the rest, accounting for nearly 70% of total inventory. They use Kanban with RFID for OR products, which accounts for 15% of total inventory, and for procedural products, a blend of Kanban with RFID and full-on RFID tagging for the remainder.
RFID-tagged Kanban locations involve systematically reordering of high-moving, low-dollar items by scanning bin cards via RFID readers. Barcode scanners are used for point-of-use and other slower-moving consumption areas. RFID is used to track consumption of owned or consigned high-dollar and specialty items at a case level by lot and item number and expiration date.

UCM determines what type of inventory technology to use based on cost/benefit analysis, according to Ilchev.
“Although it provides item-level visibility to inventory levels and expiration detail, individually tagged RFID is very expensive to implement and maintain,” he said. “Therefore, its reserved for high-dollar items and items that require chain of custody information. For example, cardiac implants and tissues are managed this way. RFID-enabled two-bin Kanban is our preferred technology in all other cases. This system provides some visibility into inventory availability (full par/half par/stockout) and is employed in most of our supply rooms. This system is relatively cheaper to implement and maintain. Barcoding provides little to no visibility and is the cheapest to implement and maintain. This is used mostly in point-of-use locations – like nurse servers or in-room OR cabinets.”
Even though case picking for preference cards represents the OR service line supply, UCM preferred RFID-enabled two-bin Kanban over barcoding and RFID alone, according to Ilchev.
“It’s a question of ROI,” he insisted. “We don’t see value in individually tagging consumable items. Our requirement here is to trigger an order when we hit the reorder point and the 2-bin RFID-enabled Kanban is much more efficient and cost-effective at doing that relative to RFID. Most barcode areas are also space-constrained and cannot accommodate the RFID technology in any form.”
UCM’s Supply Chain team also employs the use of Tableau dashboards to gather and analyze data from a variety of automated tools in a nod to generative artificial intelligence. The dashboards visually illustrate such areas as stockout trends, frequent orders, distributor unfills, and bin optimization.
“The Tableau dashboards are helpful because they provide actionable insights to all levels in the supply chain department and are designed to support analytical and operational/transactional needs,” indicated Hussam Bachour, manager, Supply Chain Systems. “The users can easily interact with (slice and dice data), dive deeper in (view aggregated and more granular data and download underlying data), and distribute (push dashboards to stakeholders using subscriptions) the Tableau dashboards without the need for technical expertise.” This means limited need for extensive training.
“Moreover, the supply chain Tableau platform supports self-service analytics,” Bachour continued. “It hosts over 50 data sources that combine data from the [enterprise resource planning] system, the Helios Requisitioning and Inventory system, GHX’s electronic data interchange (EDI) platform, Epic’s electronic medical record (EMR) system, and many other information systems. Users who had Tableau training can connect to the data sources and create dashboards and ad-hoc analytics. Tableau dashboards and data sources provide more information than the reports in the ERP because they combine data from almost all supply chain information systems. However, the reports and analytics in the ERP are helpful for specific operational/transactional needs that require timely and 100% accurate procure-to-pay data.”
UCM Supply Chain also is setting up a Web PRS point-of-use scanning system to enable clinicians in the OR to record all supplies used during a procedure to improve traceability and charging accuracy.
“This initiative is an effort to improve accuracy of supply documentation in the OR and procedural space and enhance workflow for clinicians,” noted Dinesh Gopalakrishnan, manager, Process Systems Engineering. “This project has been on our transformation map, and it is highly supported by the Periop administration, as they are looking to have better capturing of supplies and ultimately charges and revenue. We can tie the information at the point of use with preference cards and manage inventory better throughout the whole cycle. The application was developed in cooperation with our inventory management system provider – ARC. We chose web browser over Epic to simplify the implant/supply documentation interface.”
Currently, supply/implant scanning is limited to RFID-labeled items and documentation requires switching between EPIC and implant screens that takes up to three minutes per item. Under the new system, supply and implant scanning will include manufacturer barcode and 2-D RFID tags, one screen to document products with an easier item search and higher documentation rate, according to Gopalakrishnan. The system also will automate bill-only requisition, leading to an estimated $150,000 in annual savings for price accuracy, future procedure card maintenance for product changes, and increased documentation and charging accuracy for items below $150, as well as expired product alerts.
Creating, configuring and integrating this technology has seen its share of speedbumps, Gopalakrishnan indicates.
“The biggest challenge continues to be data cleanup,” he said. “Good scan rates require good back-end data on [GS1 US’] GTIN and product information. Getting that information right has been difficult, and the recent disruptions and the item substitutes they brought about haven't helped. Another challenge was getting clinical buy-in on the new workflow. We had to demonstrate that the change will yield better documentation accuracy, and also reduce documentation time in the long run to get them to agree.”
Still, Gopalakrishnan anticipates a bright future.
“Long term, we expect the function to be provided by and live within Epic, given that a lot of hospitals are starting to focus on this, but we continue to innovate and evolve our solution focused on what makes things as easy and allows for the best data integrity,” he added.

Thriving teamwork
UCM’s Supply Chain team attributes its product conversion success to cross-functional, process-interlaced sub-teams that resemble a DNA strand. Sourcing teams produce and share background information with clinical teams to approve before working with the distributor to “bleed out” old inventory to minimize waste. The Business Process team manages system data changes and updates, while the Process Transformation teams establish operational modeling for the Inventory Planning team to execute and update stock levels. Every sub-team works together to develop and carry out an end-to-end conversion checklist, according to Gopalakrishnan.
“Participating teams all have a role to play in the conversion process,” he said. “The current- state checklist was developed as a result of learnings from a past failure. The checklist itself was the product of brainstorming across different functions to determine who is involved, what steps need to be accomplished, and in what order. Then, using Smartsheet, we created a template which allows us to assign tasks to team members, send them reminders, and bring visibility to all stakeholders. The checklist is just a tool though, and the project manager assigned to the conversion essentially uses it to execute the conversion. Also, we can have the same individual work on multiple projects across different teams.”
The Process Transformation (PT) team primarily serves as internal consultants that bridge Supply Chain and Support Services, according to Bob Boyden, director, Supply Chain Operations & Transformation. PT team members function as liaisons between different teams, such as clinical and facilities, and lead cross-functional initiatives as project managers to carry out service line initiatives, such as a laboratory supply chain transformation that includes product and equipment sourcing, designing product flow, and building the supply space, he adds.
One of the hallmarks of UCM’s Supply Chain team process incorporates its Managing for Daily Improvement (MDI) infrastructure that started at the hospital and extended throughout the organization.
“The MDI process is foundational for the entire UCM organization,” Ilchev said. “Structure and process initially was driven by the Operational Excellence department; however, development of metrics, utilization, and sustainment is managed at a departmental level. For Supply Chain, MDI is part of daily operations, and we have not only sustained but also improved the process over time. As we continue to grow, the process has been replicated at each new site/group. The real challenge is recruiting, developing, and retaining the right people that could understand and embrace the way of work, and implement all Supply Chain processes effectively.”
MDI serves to identify trends and implement countermeasures through communication, accountability, and continuous performance improvement covering such issues as daily readiness, real-time management, performance management, and long-term improvement, according to Tritch. Eight areas conduct daily huddles that share insights during Tritch’s weekly management huddles. They include Business Process, Strategic Sourcing and Operations Management, which encompasses the OR Team, Process Transformation, Stat Store, Dock A Receiving, and Dock B Receiving.
“MDI is a methodology we employ across UChicago Medicine to align our teams around daily execution of key objectives,” Tritch indicated. “It starts at the front-line shift daily huddles and rolls up to manager level and ultimately the VP board. It is a way that we ensure alignment across the organization around organizational priorities and escalate problems and barriers at the front lines that can’t be addressed to higher levels until we can find a resolution. The frequency is a set cadence, but the metrics evolve based on need. If things are stable and meeting targets, then we look to new areas where there is room for improvement.”

As UCM continues to grow, Tritch’s team strives to incorporate new facilities into the mix.
“The non-acute space initially was developed as a separate division outside of Operations, which led to certain differences in process execution,” said Ron Fanning, director, Supply Chain Operations & Logistics, Ingalls/Ambulatory. “Since then, we have been working toward creating ‘One Supply Chain’ – physical locations, processes, and system are standard and provide seamless experience for the clinicians regardless of their location. The method of interaction is based on the size and type of facility – full-time presence versus on-demand versus self-managed, while still following Supply Chain-established processes and standards.
“All areas, acute or non-acute, are following the same method of measuring performance – through KPIs that are standard for all areas, specific to service satisfaction and product availability,” Fanning added.
This process also helps build trust with clinicians, according to Gabe Toledo, manager, Supply Chain Operations, Ambulatory.
“Clinicians are involved in the initial phase of on-boarding new ambulatory sites,” Toledo said. “Based on size and scope, their involvement later in the process could be very limited, based on fully Supply Chain-managed sites to self-managed with minimal Supply Chain support.”
Getting ahead of costs
To manage expenses, an organization must follow the money applied to procedures and processes. But managing expenses, as well as crises, hinges on timing. Within the last decade, UCM’s Supply Chain not only raced against time to reduce non-labor expense savings in drugs, services, and supplies, but did it without any foreshadowing of the global crisis that would erupt in 2020.
In the 10-year period between fiscal 2012 and fiscal 2020, UCM’s Supply Chain team quadrupled its annualized savings to nearly $20 million from less than $5 million, according to Tritch.
They were particularly proud of a continuous improvement project centered on bin optimization. The team sought to minimize the impact of a distributor line fee cost increase that was nearly double, decrease the total cost of ownership by increasing minimum order quantities to control labor requirements, and increase labor efficiency by reducing the number of lines ordered daily.
The team collected data to best optimize bin space in each supply room, targeting the fastest-moving items in selected supply rooms. They also created a cloud-based system to collect data and validate bin sizes per supply room. Using the data, they proved their business case, phased in process changes system-wide, and they continue to audit to monitor progress, Boyden notes.

Supply Chain’s Process Transformation team designed and implemented the project, which lasted eight months, including proof of concept, pilot, and implementation, followed by a sustainment period.
“The distributor provided product dimensions that we used to model what the future state would look like and the projected cost savings,” Boyden recalled. “This was very important in the proof-of-concept phase of the project.” He further clarified, “This is not a system-based project, but a change in our inventory model/holding pattern based on the total cost of ownership (TCO), and this process can be replicated using the TCO principle in any facility.”
Supply Chain was measuring the specific outcome over a period of intervention around moving from a “lowest unit of measure” and “minimal inventory” mindset to an “optimal” unit of measure and inventory mindset, according to Tritch.
“We didn’t want to have high turns just for the sake of high turns, but really look at when and why we need to order and create extra touches within the supply chain, balancing the trade-offs of extra inventory with labor costs and stockout risks,” he continued. The project phase was completed in the spring of 2019, roughly seven months before the COVID-19 pandemic emerged.
“We are lucky to have executed this initiative prior to the pandemic or we would have been in a much worse position, as we generally are a low-unit-of-measure/just-in-time [JIT] operation, so we have less safety stock inventory than a lot of operations,” Tritch said. “However, we’ve pivoted our strategy around both on-site and off-site safety stock and disruption management, and have partnered with Cardinal Health to be thoughtful and strategic about how and where we keep critical inventory to manage through supply disruptions. We’ve seen steady improvement in fill rates, but there are still hundreds of items on disruption daily that the team works on better managing to reduce impact and cost on our operations.”

“Osvaldo [Torres, director, Strategic Sourcing Non-Clinical] and Robbie [Brown, assistant director, Strategic Sourcing Non-Clinical] have done a tremendous job in the last two-to-three years building trust with all areas of non-labor expense to help continue the positive trajectory of annual savings. IT, Revenue Cycle, Legal, Facilities, HR, Strategy, you name it, we are a trusted partner working with them on supplier strategy and spend management. These partnerships have helped lead to creative approaches towards contracting and value creation that have driven savings in key purchased services categories.”
Brown looks ahead with promise.
“When we think about future opportunities within the services expenses, our team is focused on continuing to work with key department leaders to leverage recent consolidations of major enterprise applications as an opportunity for us to look at ancillary applications that were either redundant or can be decommissioned, along with our projected system growth as an opportunity for partners to deliver value propositions that can provide sustained value over time,” he noted. “Our team has also recently implemented more rigor around purchased services governance that, combined with the strong partnerships that we have established with our department stakeholders, will help identify new savings opportunities.”
Chain reactions
GOLD CHAIN: UChicago Medicine, Chicago, IL
SILVER CHAIN: Hartford HealthCare, Hartford, CT
BRONZE CHAIN: MultiCare Health, Tacoma, WA
UChicago Medicine Supply Chain team salutes supplier partners
Who supports an award-winning healthcare supply chain organization? UChicago Medicine’s Supply Chain & Support Services team appreciates the product and service companies that have helped them develop and improve their operations and performance. The team shines a spotlight on 10 below (in alphabetical order by company name) that have motivated and fortified them to make a difference and succeed.
AbbVie has served as a key research and collaboration partner of UChicago Medicine, and it was able to share essential PPE and N95 supplies during the height of the pandemic.
ARC Healthcare Technologies has served as a key inventory management technology partner at the center for much of our replenishment technology. They have been an innovative design partner helping us co-design new solutions in the inventory management space.
Cardinal Health has served as a strategic partner on medical/surgical supply distribution, freight and logistics management, as well as procedure packs and various branded products. Cardinal Health has been a true integrated supply chain partner through thick and thin, and has helped us drive out cost across our operations and provide critical supplies and services.
Concordance Healthcare Solutions has provided essential local disruption warehousing and distribution services during the pandemic, as well as local job growth and investment in the communities that we serve.
GHX has served as a key technology-oriented trading partner that has helped us innovate in the procure-to-pay (P2P) space and has been critical in helping us implement the Oracle cloud solution and automating manual transactions.
Medline Industries has served as a great supplier partner for med/surg supplies, service and support, and has provided critical support for hard-to-find products during the pandemic.
Stryker has helped us drive costs out of critical implant categories, and has provided great service and support for our busy Level 1 trauma center.
Supply Logistics & Procurement (SLP) has served as a local diverse provider of supply chain staffing that has been a true partner in supplying great talent to allow us to extend our supply chain services to various nonacute and affiliate sites. They’ve also been a key staff augmentation partner in critical times.
TriMedx has served as a strategic partner of healthcare technology management solutions, helping us evolve our clinical engineering processes, and capital planning and execution, along with cybersecurity of medical devices.
Vizient has served as much more than a group purchasing organization (GPO). They have been a trusted partner and connection to key networks of supply chain leaders and government advocacy. They have helped us navigate difficult times in healthcare supply chain, and provided critical analytics tools and resources, along with a strong contracting portfolio, and a foundation for our supply chain affiliate program.
About the Author

Rick Dana Barlow
Senior Editor
Rick Dana Barlow is Senior Editor for Healthcare Purchasing News, an Endeavor Business Media publication. He can be reached at [email protected].