Advocate Christ’s dream team pursues SPD quality, ‘March to Zero’ defects

Five years ago, during construction of the Outpatient Pavilion at Advocate Christ Medical Center in the southwestern Chicago suburb of Oak Lawn, executive and operating room leadership at that time made a rather curious decision against the backdrop of an industry that hinges healthcare reform to process standardization.
They chose to launch and operate a separate Sterile Processing department and team to support the 12 operating rooms inside the new building, which was located on the other side of the large Level 1 trauma hospital campus.
In essence, the leadership groups decided that two teams would perform the same function on opposite ends of the hospital campus. Unfortunately, they soon would discover that one of them was struggling. And no, it wasn’t the newest one under the direction of Yves Theodule.
By early 2015, some disturbing performance metrics surfaced during a daily communications huddle when executive and departmental leaders, clinicians and staff members convened between shifts. Through manual tracking, the group learned that SPD faced on average 650 unsterile trays every morning, incomplete trays, missing instruments and immediate sterilization use rates that exceeded 10 percent regularly, which led to high employee turnover rates. SPD consistently was playing catch-up but falling farther behind.
The huddle conversation was the wake-up call they needed. Something had to be done about the situation.
That spring, under the aegis of new executive leaders and physicians, Surgical Services Administration and SPD developed and implemented an interventional plan to improve operations and service quality for reprocessing instruments and trays.
The first step involved uniting the two SPD teams under Theodule, Manager, SPD, Surgical Environmental Services & Surgery Administration, for “standardized leadership,” reporting directly to Surgical Services Administration (SSA) and its Executive Director, Katie Sikora. SPD maintains a linear relationship with Supply Chain with one staff member (SPD calls them “associates”) overseeing the limited supplies necessary in the department, according to Theodule.
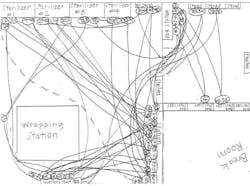
With the help of parent organization Advocate’s Operating System team for data analytics and operational support, SSA and SPD embraced the Toyota Production System concepts of process improvement and lean methodology. They used process flow mapping, spaghetti diagrams and time studies to reorganize the department into an efficient and safe work area, according to Sikora. Throughout much of 2015 and 2016 as daily responsibilities continued, they assessed staffing levels compared with service demands, manual data defect collection in the OR and SPD, tray backlogs and IUSS rates. From that extensive work the hospital’s executive team clearly understood that SPD required additional investment in labor and knowledge support that included electronic reporting capabilities, priority case picking for procedures, instrument reprocessing staff scheduling better aligned to case demands, structural education and increased certification requirements for SPD associates, Sikora noted.
COO Matthew Primack expressed pride in how SPD approached and handled the challenges that lay ahead for them during that time.
“After identifying several opportunities to improve, the SPD leaders designed and implemented a broad transformation plan which included staffing model renovation, enhanced equipment storage and maintenance, creative process flow mapping, and innovative and comprehensive safety measures,” Primack said. ‘Even more impressive than these complicated interventions, was the overhaul of culture by engaging associates to become a part of the solution and hold themselves accountable for change. There was an overwhelming shift to the concept of TEAM and a common goal to bind the department together. This effort has served as a model for our organization to successfully implement change with a rapid and sustainable method.”
- Volumes include Advocate Children’s Hospital-Oak Lawn Campus
- 2018 data updated through February 18, 2018
- 2018 data updated through February 28, 2018 Source: Advocate Christ Medical Center, April 2018
Sikora established the contextual relationship between SPD and the OR, which fueled the motivation to change.
“More than just a revenue generator for a hospital, operating rooms are a source of physician, patient, and associate satisfaction — or dissatisfaction — depending on the operational efficiencies of the OR,” she said. “ACMC strives to provide the best care to its patients, best place to practice, and best place to work.” After completing a strategic review of operational efficiency, the group conducted a gap analysis and initiated workforce teams to explore SPD, pre-surgical testing, OR turnover times and surgery access.
“Through these work teams SPD leadership met with executive leaders and a true understanding of the importance of SPD’s needs were realized,” Sikora continued. “SPD is the foundation of surgery. To provide the best services to our surgeons and patients we needed to create the best SPD where we could ensure that the right instruments are delivered to the right surgeon/patient, at the right time with no defects.”
With an effective plan in place, the SPD team began what it called its “March to Zero,” as in “zero defects,” to improve what it feels is “crucial work being done in the ‘heart of the hospital,’” Sikora recalled.
“Our SPD continues to succeed because we work together, we encourage staff to put their best foot forward, and we understand the importance of our job, ‘Serving Patients Diligently” or SPD,” she said.
Throughout SPD’s entire performance improvement process, Advocate Christ’s “dream team,” under the leadership of Sikora, Theodule and Perioperative Project Manager Parisa Yasmin, focused on one specific goal that served as purpose: The patient. The team’s mantra: The SPD is where it all begins.
For recognizing and tackling the challenges they faced, recruiting executive leadership to support their proposed solutions, and changing how they operate with the right attitude, Advocate Christ Medical Center’s SPD team earned Healthcare Purchasing News’ 2018 SPD Department of the Year Award.
Out with the old
Armed with a spaghetti diagram illustrating SPD workflow that resembled a cord-strewn, 1970s-era sound studio for a heavy metal album recording, Theodule’s team recreated the technician’s workspace with marked floors to improve travel paths, cart assembly and supply searches in sterile storage.
Simple changes led to significant improvements. SPD standardized the tools and resources at each workstation with easy visualization cues. Floor and priority carts sport visual cues and alerts, too, so that SPD knows when rapid turnovers occur and one-of-a-kind trays are needed quickly. SPD also categorized and rearranged what had been disorderly storage areas, using clear labels and pegs with Kanban cards.“Creating this work space provided increased accessibility to help achieve increased efficiency and accuracy when comprising instrument trays,” Theodule said. “It provided all equipment and items necessary for the technician to work within their workspace, eliminating the need to leave.”


SPD organized loose inventory on pegboards and in bins. The peg boards and bins are displayed in category and alphanumeric order, making it easier to replace instruments when needed. SPD’s Non-Conforming Technicians maintain the pegboards and bins, conducting daily inventory and ordering as necessary.

If an instrument is on back order, and a tray becomes incomplete, the tray is tagged with an orange dot and placed on the Non-Conforming cart, which alerts the Non-Conforming Technician that a critical instrument should be replaced. When critical instruments are missing from a tray and a rapid turnover isn’t achievable, SPD may use a “gold tray” instead, Sikora explained. These trays were created as supplemental PAR levels or as a necessary back-up for high-volume or specialized trays. SPD’s gold tray system enables the department to provide complete and functional trays to the OR, despite instrument backorders, without delaying surgeries, she added.
SPD established a two-bin system with Kanban cards for a visual replenishment cue to reorder product. To assist the OR upstairs the team created an immediate-use safety stock zone accessible to the OR staff to eliminate the opening of full trays for one or two items that may be dropped during a case.
Sikora noted that Supply Chain already had been using the two-bin Kanban system in the patient care areas with some degree of success so implementing a higher-cost software system wasn’t considered as a potential and preferential solution.
“The two-bin Kanban system was found to be an optimally efficient method to control and create continuous replenishment of stock through a visual cue — empty bin — that communicates the need to replace stock in a cost-effective manner prior to it being fully depleted,” she said. “It was determined that software was not necessary, as the two bin Kanban system is a truly effective and optimal method.”
Loaner trays represent more than 20 percent of the trays SPD sterilizes, so the team uses an electronic Casechek Loaner System to link loaner technicians, vendor sales representatives and OR staffers when checking these trays in and out. SPD color-codes and wraps these trays with appropriate identification for surgical cases, which gives the OR its own visual indicator, according to Theodule.
“We hope to reduce the percentage of loaner instruments through continued partnership with our surgeons to create standardized tray system availability,” Sikora indicated.
Advocate Christ Sterile Processing Associates
Yves Theodule, Manager, CRCST, CSPDT, CIS, CER CHL
Sheree Coley, Educator, CRCST, CIS
Micheal Vinson, Coordinator, CRCST, CSPDT, CIS, CER
Lisa Sanders-Triggs, Coordinator, CSPDT
Micheal Hardy, Coordinator, CSPDT
Renea Spivery, Coordinator, CSPDT
Lenore Williamson, Non-Conforming Tech, CSPDT, CSIS
Jennafer Lloyd, Non-Conforming Tech, CSPDT
Kristen Berry, SPD Lliason, CST
Lena Aleksich, SPD Lliason, CST
Christine Bardach, Tech II, CRCST
Glenda Craig, Tech II, CRCST
Paul Harjung, Tech II, CSPDT
Denise Slaughter, Tech II, CSPDT
Bridget Porter, Tech II, CSPDT
James Tallon, Tech II, CRCST
Phillip Kwasny, Tech II, CRCST
Dora Galvin, Tech II, CSPDT
Dwayne Walton, Tech II, CSPDT
Debra Fields, Tech II, CSPDT
Michele Harrington, Tech II, CSPDT
Melaine Irving, Tech II, CSPDT
Jessica Moore, Tech II, CSPDT
Renne Wozniak, Tech II, CRCST
Yolanda Gerena, Tech II, CRCST
Felecia Jackson, Tech II, CSPDT
Dina Brooks, Tech II, CSPDT
Vanessa Perry, Tech II, CSPDT, CSIS, CFER
Jennifer Edwards, Tech II, CSPDT, CSIS
Kayode Oluwatobi, Tech II, CSPDT
Luz Quintos, Tech II, CSPDT
Terri Offord, Tech II, CRCST
Dorothy Landrige, Tech II, CRCST
Charity Wilkes, Tech II, CSPDT * Passed away
Danielle Bryant, Tech II, CSPDT
Sheila Lavin, Tech I, CRCST
Raul Gomez, Tech I, CSPDT
Samantha Green, Tech I, CSPDT
Larinda Mcclinton, Tech I, CSPDT
Mykeal Hood, Tech I, CSPDT
Kettia Antoine, Tech I, CSPDT
Kimberly Coleman, Tech I, CSPDT
Sandra Hicks, Tech I, CSPDT
Brooke Kozi, Tech I, CSPDT
Phamey Alexis, Tech I, CSPDT
Heidi Standifer, Tech I, N/A
Chiquita Patterson, Tech I, N/A
Martikeika Hudson, Tech I, N/A
Felix Aguayo, Tech I, N/A
Lakesha Feaster, Tech I, N/A
Tasha Hamm, Tech I, N/A
Stephanie Joyner, Tech I, N/A
Monica Brown, Tech I, N/A
Darly Louis-Charles, Tech I, N/A
Armani Jones, Tech I, N/A
Shareese Kindle, GI Reprocessing Tech, CFER
Juana Soto, GI Reprocessing Tech, N/A
Selena Diggs, GI Reprocessing Tech, N/A
Source: Advocate Christ Medical Center, April 2018
Marching to zero
The SPD Workgroup, composed of OR, SPD, Nursing, Finance and Project Management executives and associates, launched its “March to Zero” drive toward high reliability, quality and safety with zero defects in April 2016. Sikora represented the administrative and financial resource liaison with the C-suite and worked with Cindy Mahal-van Brenk, Vice President of Surgical Services for Advocate Health Care, to explore savings opportunities, staffing to demand and building relationships. Theodule oversaw day-to-day SPD issues and long-term OR-SPD strategic goals, while Yasmin focused on project management between the two departments. The group met weekly to target rapid improvement, Yasmin indicated, and as goals were met over time the frequency tapered to monthly reviews led by Matthew Balog, Director of Business Finance for Surgical Services, and Lenore Williamson, SPD Non-conforming Technician.
The SPD Workgroup defined “defect” as any quality issue within a tray that is avoidable, such as a missing instrument, broken instrument, bioburden or hole in the wrapper. “As we all know, a defect within a tray can be disastrous for patient outcomes, both with risk of infection and possible procedure delays,” Sikora noted. “This all could result in extended periods of surgical time for patients under anesthesia, as well as an increased length of stay and complication rate; all which directly affect the cost to the institution vs. reimbursement rates.”
To generate useful data for pursing zero defects, SPD replaced its “antiquated” electronic tracking system with a Censitrac electronic monitoring system to collect and update instrument defect reports and review and assist with necessary countermeasures and interventions, according to Sikora. The new system opened an immense opportunity to monitor many other sub-processes that were in the works for quality improvement, including instrument maintenance, case cart pulling, newly designed rapid turnover protocol, tray updates and physician preference card updates, she continued.
“We needed to hardwire protocols and processes before we implemented an updated electronic instrumentation monitoring system in all attempts to do it right the first time!” Yasmin said.
That’s why Yasmin worked within the huddle to validate daily defects, tallied finalized monthly outcomes in collaboration with the SPD team, completed real time one to two weeks post-month for full review with the SPD Work Group, and reported out monthly to the Governance Committee for discussion, Sikora noted. “The SPD Leadership team reviewed, coached and created counter measures in real time at every daily huddle with their teams input,” she added.
Because of the success SPD experiences with Censitrac monitoring, the OR areas are implementing the system this year, too, according to Sikora, as a way to take optimal patient care to the next level. “SPD is always reviewed for instrument defects, but [defects] also needto be reviewed in all operative/touch point areas as well,” she continued. Sikora called the handling and reprocessing of instruments a “living, breathing process, constantly being reviewed for improvement.” In fact, perioperative staff ensures all instruments are free from blood, tissue and bone during each operative procedure as well as spraying all soiled instrumentation with an enzymatic foam to help decrease bioburden and biofilm before transport to the SPD decontamination area, she added.
“A good and engaging relationship with SPD and the OR is vital to successful patient outcomes and quality instrumentation,” Theodule insisted.
The OR sterile core houses a number of “tickie racks” that hold individual peel packs as part of the OR “safety stock,” much like a retail outlet will display product.
“We call them ‘tickies’ as they are a catchy name,” Yasmin said. “These tickies on the safety stock of the OR are the high use and/or rare instruments necessary for procedures, just an arm’s length away from the OR. Having these available decreases the need to open additional trays, IUSS, and the valuable procedural time it could take to replace one surgical item on the field.

Through the SPD Workgroup’s efforts and staff performance, SPD slashed their average tray backlog to 20 last year from roughly 650 unsterile trays on average two years earlier. SPD defines a tray backlog as any tray awaiting sterilization prior to 8 a.m. Backlogs, of course, generally elevates IUSS rates. Courtesy of the considerable backlog reduction, SPD has reduced IUSS rates to 1.8 percent last year from 8.3 percent the year before, which also decreases the amount of time the patient could be under anesthesia related to instrument needs during a case, Sikora noted.
Productivity has soared, too, starting with staff turnover dropping to 10 percent last year from 45 percent the year before due in part to consistent workflow, clarity of work functions and a team-centered environment that created a more content staff, according to Sikora. Prior to the process redesign, SPD infamously maintained the highest staff turnover rate of all departments at Advocate Christ, Sikora admitted.
“We currently utilize a productivity measure that looks at budgeted FTEs to number of items processed per day,” Sikora said. “Our goal is to be 99 percent to 102 percent productive per day. In 2017, SPD ended the year at 116.8 percent productive and nearly 6,000 hours under expected labor hours for the year while still continuing to provide safe quality trays. We have increased tray productivity by approximately five trays per hour per technician.”
Pulling teams together
SPD counts communication as the key to customer service so the team starts each shift with a “communication huddle.” During the huddle, the outgoing shift debriefs the incoming shift on the needs of SPD and the OR. The huddles also serve as an interaction point between team members working on different shifts, further cementing the entire department as a unit and prepping for upcoming surgical demand, asking clarifying questions and providing support for one another.
SPD created four liaison roles with the OR where two work in SPD on the communications team and the other two work in the OR. The surgical liaison also communicates to the SPD liaison when surgeries have been added for the day, and if specific trays need rapid turnover based on the OR schedule.
Solidifying SPD’s partnership with the OR definitely improved the customer service relationship, Sikora insisted. “SPD leadership and associates round in the ORs,” she said. “They have a visible presence with both the OR team and physicians. The OR team sends down trays when they are not used and houses less in the OR cores since we have made these changes. They are confident that SPD will have what they need for them when then call. We are all one team working together to provide care to our patients, and it is a noticeable difference from years prior. As one of our SPD leaders always says: One team, one dream!”
Sikora assures that Advocate Christ’s SPD-OR fusion can be replicated by those departments looking to emulate their example.
“First, I would highly suggest pulling together all of your key stakeholders to determine what processes do you need to work on,” she advised. “At ACMC, we realized that we had several opportunities for improvement. The most important was to fix our foundation. If the SPD associates could not find the tools they needed to do their job how could we expect anything else to change? Your house is only as strong as your foundation. Second, it is very important that you listen to your key stakeholders and your front-line associates. They are at the sharp end of the process.
“Far too often leaders make changes because they think they know what the customer or associate wants,” she continued. “Take time to hear your teams, engage with your teams and create a plan together. After the plan is created and implemented, review that plan daily in huddles for opportunities to improve on it. If you get it 80 percent right when you first implement a plan, then that’s a success. Each hospital will have different opportunities for improvement. Remember as you do implement change to celebrate your wins no matter how small. Celebrating these moments as a team only helps to sustain the momentum.”
Sidebars:
About the Author

Rick Dana Barlow
Senior Editor
Rick Dana Barlow is Senior Editor for Healthcare Purchasing News, an Endeavor Business Media publication. He can be reached at [email protected].