Bundle up for better patient care

Bundles are powerful weapons in the battle against hospital-acquired infections (HAIs). It is a simple concept, with simple steps, but bundles can help to deliver optimal patient care. A bundle usually is comprised of three to five steps. It has been proved time and again that, when these steps are performed together and consistently (read: every single time), patients benefit.
To be clear, a bundle is not a checklist but a set of processes, based on best practices, that is a certain person’s or team’s responsibility to perform at a certain point and time, for example, during central-line insertion. There is a temptation to make additions to a bundle, but the danger is making the bundle unwieldy, which means a person or team is less likely to comply.

Kraus added that those in the emergency departments “strive to know what the care bundles are for the inpatient team and to begin those steps at the point of entry when the patient enters into the healthcare system. Collaboration between the emergency department and our inpatient colleagues is essential to have smooth transitions and provide optimal care. The Emergency Nurses Association provides the emergency-department nurses with tools and education to provide excellent care and allows them to practice with more confidence. That leads to infection prevention in many aspects of patient care encompassed by the patient-care bundles.”

“The key thing about bundles is that, while each individual element is a best practice, they must be performed together and consistently,” stated Wright. “Bundles tie related interventions together into a single, structured, step-by-step protocol that is easier to remember. By pulling them all together into a bundle, it’s easier to ensure that each piece is done, with a greater impact on patient care.”
There is no one-size-fits-all bundle. Wright noted, “Each HAI has an associated bundle that has been studied and validated.” She provided an example. “For central-line–associated bloodstream infection (CLABSI), the bundle includes hand hygiene, use of chlorhexidine gluconate for cleaning the insertion site, maximal barrier precautions during insertion, optimal site selection, daily review of line necessity, and scrubbing the hub. The strength in bundles lies with their relative simplicity. Each element is small, precise, and straightforward, lending itself to ease of use as well as consistency.”
Wright explained how her unit at Duke Regional Hospital keeps on track. “In our unit, we educate about bundles during our yearly ‘Bundles Bashes.’ We developed the Bundle Bash about seven years ago in response to higher rates of infection. The event has a different theme each year, such as Monster Mash around Halloween or March Madness in the spring. We try to make it as festive as possible by providing snacks and celebrating our successes. While Bundle Bashes are typically annual, if we notice drift in practice or have a change in our infection rates, we may have one early. At the end of the Bundle Bash, we are all on the same page about the value of bundles and how to make them a part of the care we provide every patient every day.
“Each session is only an hour long, with a variety of activities. We review the various bundles and use audit results to focus on any specific areas of concern. We try to make it fun to engage staff. Being silly about a serious subject can grab attention and improve attendance and learning. For example, we changed the lyrics to Row, Row, Row Your Boat to be Scrub, Scrub, Scrub Your Hub. The song lasts at least 15 seconds, which is the amount of time that you’re supposed to scrub the hub prior to accessing a central line.
“That said,” continued Wright, “infection prevention is not always fun and games.” The team makes it personal, never forgetting they are working with humans not just case numbers. “We find that thinking of infections as rates or numbers can be really abstract and impersonal. Sometimes we must go beyond numbers to discuss individual patients and how we could have done a better job caring for them. ‘We could have prevented Ms. X from harm’ is a much different thought process than ‘Our infection rate is X.’ Knowing the direct impact we have on our patients’ health and safety makes us look at infection prevention a bit differently. We do the bundle because we want our patients to have the best care and the best possible outcomes.”
Wright and her team practice what they preach, as evidenced by results. Their unit “has outperformed the mean for National Database of Nursing Quality Indicators for catheter-associated urinary tract infection (CAUTI), CLABSI, and hospital-acquired pressure injuries (HAPI) for eight quarters, July 2016 through June 2018.” They experienced zero HAPI stage 2 or greater during the two-year period; zero CLABSI for one year, July 2017-June 2018; zero CAUTI for four of the eight quarters, July 2016-June 2018; no central-line infection for more than a year; no CAUTI for five months. They are the 2019 recipient of the Circle of Excellence Award from the American Association of Critical-Care Nurses, which will be presented at the National Teaching Institute & Critical Care Exposition, May 20-23, in Orlando, FL.
Vanquishing VAP
Reducing rates of ventilator-associated pneumonia (VAP) by using a bundled approach is supported in published scientific literature. One example is a study by Resar et al.1 The results found, “For the 35 units that consistently collected data on ventilator bundle element adherence and VAP rates, an average 44.5 percent reduction of VAP was observed.” The authors concluded, “The observations seem sufficiently robust to support implementing the ventilator bundles to provide a focus for additional change in ICUs.”1
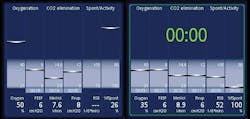
When a patient must be on a ventilator, it is best that he or she be weaned off it as quickly as is feasible. The longer a patient is on the ventilator, the more likely VAP can develop. Alexander Starcevic, Director of Marketing, described how their product, Hamilton Medical AG ventilators, offers two technologies that support VAP-bundle recommendations. “In the Institute for Healthcare Improvement’s bundle, the daily assessment of readiness to extubate is one of the five elements of care for prevention of VAP. To make this assessment easier for the caregiver, Hamilton Medical ventilators display the Vent Status panel. This dynamic graphic displays six parameters related to the patient’s ventilator dependence, including oxygenation, CO2 elimination, and patient activity. Floating indicators moving up and down within the columns show the value for a given parameter (Figure 1). When the indicator is in the light blue weaning zone, a timer starts, showing how long that value has been in the weaning zone. When all values are in the weaning zone, the Vent Status Panel is framed in green, indicating that spontaneous breathing trials should be considered. The panel supports the clinician in assessing the patient’s readiness to wean and can be configured to the institution’s individual weaning protocol.
“The leakage of oropharyngeal and nasopharyngeal secretions or gastrointestinal contents past the endotracheal tube is a causative risk factor in the development of VAP,” explained Starcevic. “Multiple studies have shown that continuous cuff-pressure control can help to reduce this risk and decrease the incidence of VAP (Figure 2).” Starcevic said the IntelliCuff cuff-pressure controller continuously measures and automatically maintains the set cuff pressure during mechanical ventilation with cuffed endotracheal tube or tracheostomy. “The clinician sets the target pressure relative to the peak airway pressure, as well as minimum and maximum values. IntelliCuff then automatically adjusts the cuff pressure within these ranges. To always be on the safe side, the pressure never exceeds 50 cmH2O.” IntelliCuff is available on all Hamilton Medical ventilators either as an integrated option or as a standalone device.

CLABSI, CAUTI, HAP, SSI
Consistency in completing a bundle’s required steps is the key to success. Angela Zuick, Director of Clinical Education, Medline, explained that their infection-prevention solutions are designed to be intuitive and efficient so as to reduce variance in practice. “From our pocketed drape with visual cues for CLABSI prevention to our one-layer CAUTI tray and oral-care kits, we work alongside clinicians to develop an easy-to-adopt process that combines clinical thinking with product and educational resources to drive clinical and operational outcomes. A few examples of areas we’ve focused on designing bundled solutions for include BSI, CAUTI, hospital-acquired pneumonia (HAP), and surgical-site infections (SSIs).”
“Urinary tract infections are one of the most common HAIs, and about eighty percent of them can be attributed to an indwelling urinary catheter,” said Zuick. “The ERASE CAUTI Bladder Bundle is the first line of defense in CAUTI prevention and is the foundation of a ‘smart’ Foley approach, enabling clinicians to influence outcomes by assessing bladder function, then leveraging the right alternatives at the bedside.”
Another one of Medline’s bundles focuses on helping to reduce SSIs by engaging patents prior to surgery. Patients are provided with the necessary products and step-by-step instructions to ensure they are prepared for their appointment. “Medline’s customizable Ready.Set.Prep combines products and multimedia resources to assist patients in reducing the risk of acquiring an SSI,” explained Zuick.

“As a strategic partner, Medline is dedicated to working with hospitals to help reduce their infection rates,” continued Zuick. “One example is our partnerships with customers to reduce HAP, with a focus on non-ventilated patients. We collaborated with one academic center on the West Coast to implement oral care for all patients. This helped lead to a decrease in number of HAP, HAP sepsis, and mortality. Additionally, Medline worked with Nebraska Medicine to standardize clinical education around best practices to reduce CAUTIs.”3
Devising a system for medical devices
Erin Broeske, Senior Marketing Director, Stryker’s Sustainability Solutions Division, advised Healthcare Purchasing News that health systems should look at their medical devices as part of their comprehensive infection-prevention bundle, since one quarter of HAIs are device-associated infections.5 “Disinfection and sterilization of reusable medical equipment is critical to prevent the spread of bacteria between patients. Hospitals train staff to use specific cleaning procedures for each reusable device; however, the multitude of different devices used in each facility, and staff turnover, make implementing a consistent process across an organization challenging,” noted Broeske.
“Replacing reusable devices with single-use devices (SUDs) is one solution that helps offer confidence that every device will be ready for patient use,” continued Broeske. “Some health systems hesitate to make the swap because of the perceived cost and waste increase. However, it can cost a health system roughly $20,000 to treat a single HAI.4 Stryker’s Sustainability Solutions Save Simply ECG leads are an SUD designed to decrease the infection-prevention concern associated with reusable ECG leads, helping health systems save the potential cost of treating one HAI. In addition, the Save Simply ECG leads seamlessly integrate with a third-party reprocessing solution that can further drive cost control and environmental-waste reduction.”

Broeske pointed to two recent studies demonstrating the role single-use ECG leads played in a comprehensive infection-prevention bundle. St. Anthony’s Medical Center, St. Petersburg, FL, reported a 70 percent decrease in combined methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and Acinetobacter HAIs and a 30 percent decrease in Clostridium difficile when disposable ECG leads were added to the hospital’s infection-control bundle. In addition, Bon Secours St. Francis Hospital, Midlothian, VA, reported a twenty-three–month zero infection rate when using disposable ECG leads as part of their infection-control bundle. When success in telemetry and the intensive-care unit was noted, surgical services began using disposable leads and achieved a forty percent decrease in SSIs.5
Gary Rabinovich, Marketing Director, Clinical Procedural Solutions at Owens & Minor Inc, Halyard, explained that the reason bundles play an important role in preventing HAIs such as CLABSI is because they help clinicians maintain a consistent and standard set of practices, so that components of the bundle remain sterile, contributing to better patient outcomes. Rabinovich noted how their product supports bundling. “Halyard’s Clear Sequence kits are a customizable product delivery mechanism and aseptic drape system that support the establishment and standardization of a central-venous access-device maintenance bundle.”

Rabinovich described how the product works. “Clear Sequence is designed with ten clear pockets on a single drape, five on an upper row and five on a lower row. While the clinician is using the components on the top row, the lower-row components remain covered by a flap, ensuring that they remain sterile. The components themselves are logically arranged from left to right, in the order they are needed according to protocol, and the pockets are sized to accommodate most brands of each component, per Infusion Nurses Society guidelines, giving hospital staff free reign to choose based on their preference. Customized, step-by-step illustrations of a hospital’s protocols can be attached to the flap so clinicians can follow them while performing the procedure.”
The bottom line
Bundling is good for improving patient outcomes, good for helping to keep healthcare workers consistently on track with evidence-based best practices, and good for the hospital’s pocketbook. The bottom line is bundle up for a win-win plan of action.
References:
- Resar R, Pronovost P, Haraden C, et al. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm Qual Patient Saf. 2005 May;31(5):243-248.
- Lorente L, Lecuona M, Jiménez A, et al. Continuous endotracheal tube cuff pressure control system protects against ventilator-associated pneumonia. Crit Care. 2014 Apr 21;18(2):R77.
- Gross R, Nelson A. Decreasing CAUTI rates in the ICU patient. https://www.medline.com/wp-content/uploads/2018/11/Nebraska-Medicine-Poster.pdf. Last accessed April 2, 2019. Am J Infect Control. June 2018. Abstract.
- Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2014 Mar 27;370(13):1198-1208.
- Brown DQ. Disposable vs reusable electrocardiography leads in development of and cross-contamination by resistant bacteria. Crit Care Nurse. 2011 Jun;31(3):62-68. http://ccn.aacnjournals.org/content/31/3/62.full?cited-by=yes&legid=ccn;31/3/62&_sm_au_=iVVN4S8NL560npLM. Last accessed April 3, 2019.
About the Author

Susan Cantrell
Susan Cantrell is Infection Prevention Editor for Healthcare Purchasing News.