Not Scanning UDI: What Are You Missing?

In this month’s column, we revisit a perennial topic: Why aren’t hospitals taking more advantage of the fact that most medical device packaging labels now contain barcodes with US FDA-mandated unique device identifiers (UDIs)? Scanning UDI barcodes provides both the device identifier (DI), a unique code assigned to specific products at different packaging levels, and an application identifier (AI) that includes key production data, such as expiry date and lot, batch, or serial number. Scanning is particularly valuable today as hospitals continue to deal with product shortages and manufacturers and providers seek ways to share more inventory and consumption data to advance demand planning and forecasting.
When asked why scanning is not more prevalent, many providers blame their lack of scanning on poor barcode quality and/or too many barcodes on a package making it hard to know which one to scan.
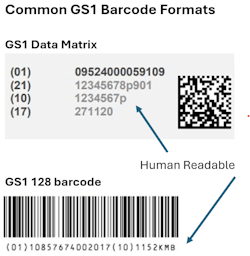
But those arguments have been disputed by research conducted by GS1 US. In 2021, the standards organization found that more than 70 percent of providers were able to scan both the GS1 128 (linear) and data matrix formatted barcodes, the most common barcodes found on medical devices. More recently, GS1 US conducted a “Scanathon” at a large, multi-state healthcare system, which further contradicted some of those arguments.
Here’s what they did:
- Scanned more than 12,000 barcodes at multiple packaging levels for more than 6,280 unique products in the warehouse/fulfillment center, and in the inventory areas for operating rooms, Cath labs, and angioplasty labs.
- Used a combination of newer and older scanners, each programmed to identify any kind of barcode.
Here’s what they found:
- The majority of products were labelled with GS1 formatted barcodes (primarily 128 or data matrix).
- Half of the products had what is considered a single barcode (including packages with the same barcode printed multiple times or multiple types of GS1 barcodes but each with the same information embedded).
While the study contradicted the two most common excuses for not scanning, there are still opportunities for improvement. For example, the older scanners were harder to use, especially in low light environments. Newer scanners, on the other hand, could often read products on higher shelves, even when the scanner was held by someone on the floor. Some labels could also be higher contrast or printed on less reflective paper to make them easier to scan.
In other cases, providers may need to program scanners to select the information they want captured and ignore the rest. It can also help to train personnel about why scanning is important and how to identify the right barcode.
Providers have also called on manufacturers to limit the use of two stacked linear barcodes (one with the DI and the other with the AI) as it requires two scans, which can be challenging in fast moving procedural areas. The data matrix is becoming increasingly popular as it can hold more information in a smaller space.
Finally, one of the most common barriers to change in healthcare is added cost, even though the cost of scanners has been coming down. Perhaps the more important question is: “What is the cost of not scanning?”
- How many products expire because hospitals are not effectively reading and managing expiry dates in the UDI?
- How many products are documented as miscellaneous because they were not scanned and properly identified for patient charging and capture in electronic health records?
- How many recalled products are still on the shelf and potentially a patient safety hazard because they are not accurately scanned and identified as such before use?
These are just a few examples of where scanning can make a critical difference.
About the Author

Karen Conway
CEO, Value Works
Karen Conway, CEO, ValueWorks
Karen Conway applies her knowledge of supply chain operations and systems thinking to align data and processes to improve health outcomes and the performance of organizations upon which an effective healthcare system depends. After retiring in 2024 from GHX, where she served as Vice President of Healthcare Value, Conway established ValueWorks to advance the role of supply chain to achieve a value-based healthcare system that optimizes the cost and quality of care, while improving both equity and sustainability in care delivery. Conway is former national chair of AHRMM, the supply chain association for the American Hospital Association, and an honorary member of the Health Care Supplies Association in the UK.